
If you’re a regular on this blog, you probably know that Peter Sheath and Matt Robert have enough knowledge, compassion, and common sense about addiction and recovery to lead us to a far far better world. I’ve grabbed these gems from their comments to a recent post. If you’ve already read them in context, well read them again. If not, now’s your chance.
Peter Sheath:
 I feel like there is an amazing amount of synchronicity going down, especially between you [Marc], Matt and li’l ol’ me. I can almost guarantee that I will have had my interests stimulated by a client, book, lecture or simply talking to someone and, a few days later it will be there in your blog and Matt will have made one of his beautifully eloquent comments on it. This may not sound so apparent at first but please bear with me.
I feel like there is an amazing amount of synchronicity going down, especially between you [Marc], Matt and li’l ol’ me. I can almost guarantee that I will have had my interests stimulated by a client, book, lecture or simply talking to someone and, a few days later it will be there in your blog and Matt will have made one of his beautifully eloquent comments on it. This may not sound so apparent at first but please bear with me.
Over the past couple of years I’ve been doing a lot of thinking, talking and research around this whole co-occurring conditions/dual diagnoses thing. I think we, organisationally, have got astonishingly good at not dealing with it. We love to have these imaginary silos that we place people into, develop manuals and protocols to either keep them there or embargo them from going there. We’ve even developed competency/accountability frameworks, skill-sets and governance systems that ensure that, supposedly, the right person is working with the right person, at the right time, in the right place.
The trouble is that it mainly creates confusion, uncertainty, apartheid and exclusivity. Only the other day I received a phone call from a friend who is managing a substance misuse team for people with complex needs. He had been asked to develop a “criteria” for the people his team would be working with. I said that I’m very sorry but I really do not believe in having criteria for people we do or don’t work with and everybody who comes to substance misuse services for help will have complex needs. Turns out that he is of exactly the same mind but has to do it because that’s what he’s been instructed to do.
Doing things in this way means that we often screen more people out than we do in and I have real difficulties understanding why we continue to do it. Jordan Peterson’s 12 rules for life, motivational interviewing, open dialogue, ACT, CBT, person-centred counselling, narrative exposure, etc. are all transdiagnostic and probably work best under the collective umbrella of the therapeutic relationship.
I’m currently working with a paying client who has had a lifetime of psychiatric diagnoses and various dependencies. He came to me because he had approached his local alcohol service looking for a community alcohol detox. The detox would need to fit around his work, because he works for himself and is the only employee. He was drinking at least a 750-ml bottle of vodka every day and was getting increasingly desperate and depressed. The service said that, because of his underlying mental health problems, levels of alcohol use and not being able to take time off work they couldn’t help him! I know it beggars belief, doesn’t it? I negotiated a course of Librium with his GP, involved his mother and his local pharmacist in the plan (open dialogue), then did some motivational interviewing type interventions to boost his confidence and ensure that getting sober was the right thing to do. We arranged a daily telephone check-in and weekly face to face, with myself, and I taught his mum and him how to do blood pressure monitoring. He agreed to call in to the pharmacy if his BP raised or reduced by 10.
Got a phone call last night to say that his detox had finished a week ago and he is now 21 days sober. He has struggled a bit because the weather over here has been lovely and he has an association with sunny days and sitting outside the pub drinking beer. He has used some psychotropic meds sparingly, because he does get worried about his anxiety levels, panic attacks and past psychoses. I’ve also been teaching him mindfulness-based meditations, relapse prevention and managing his mental health. We’ve developed a really good therapeutic relationship based on trust, autonomy, prosocial role modelling and hope. We’ve also focused on very small steps, although he is always wanting to make massive leaps. Fingers crossed.
Matt Robert:
 Hey Peter!! It keeps coming back to this, doesn’t it? It takes a village…but a coordinated one that meets the needs of the individual as well as the tribe. Your sentence captures it all:
Hey Peter!! It keeps coming back to this, doesn’t it? It takes a village…but a coordinated one that meets the needs of the individual as well as the tribe. Your sentence captures it all:
“We’ve developed a really good therapeutic relationship based on trust, autonomy, prosocial role modelling and hope.”
There has to be autonomy, agency… individuals need to feel in control or we don’t feel safe. I have to trust my fellow participants, the method, the goal, because I’m not going to stick with a process of arduous change if I don’t believe in it. And none of it is gonna work if I don’t feel like I’m in a sharing, connected, reciprocal relationship with the humans who are helping me. Something all effective recovery traditions have in common. All human endeavor, for that matter.
The thing about open dialogue that is so simple and compelling is that it is the same model humans have used to cooperate, help each other, and progress throughout history. It’s getting all the stakeholders, the people who care, in the same room, on the same page. It’s putting the puzzle that’s fallen apart back together.
We all know how to do this because it is a human thing, not an “addiction” thing. Addiction is a proxy for meaningful relationship.
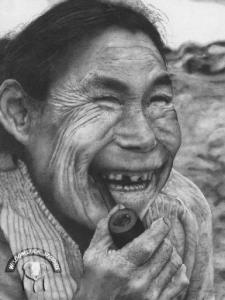
 of ice. When spring arrives, it is of no use to try to clear it up all at once. The only thing to do is to let each layer appear one after another as the higher chunk thaws. So one layer thaws and is cleared away, then another, then another. No one can force their way prematurely to the bottom of the heap, but they can rest assured that every layer will finally be revealed and dealt with.
of ice. When spring arrives, it is of no use to try to clear it up all at once. The only thing to do is to let each layer appear one after another as the higher chunk thaws. So one layer thaws and is cleared away, then another, then another. No one can force their way prematurely to the bottom of the heap, but they can rest assured that every layer will finally be revealed and dealt with. This parable corresponds beautifully with the Inuit concept of time. I have come to understand this. From the birth of man and consciousness, in earlier agricultural societies, time was circular. The rhythm of life was cyclical, from the beginning of life in spring through growth, harvest and finally death. Death was followed by rebirth, for nature and for man. The cycle would start all over again. The industrial revolution changed our concept of time, nature did not dictate it any more, but production lines did. Time became linear, just like production and progress. Peak performance was always in demand. Be productive! Act now! Consume now! Be happy now! And be greedy!
This parable corresponds beautifully with the Inuit concept of time. I have come to understand this. From the birth of man and consciousness, in earlier agricultural societies, time was circular. The rhythm of life was cyclical, from the beginning of life in spring through growth, harvest and finally death. Death was followed by rebirth, for nature and for man. The cycle would start all over again. The industrial revolution changed our concept of time, nature did not dictate it any more, but production lines did. Time became linear, just like production and progress. Peak performance was always in demand. Be productive! Act now! Consume now! Be happy now! And be greedy! The old Inuit concept of time sees no time spent, no time wasted, no time gone. Time arrives. Time only arrives. Each and every moment we receive the gift of time to be added to all the gifts of time already received. Yes, nature is cyclical, yet still unpredictable; the variations in weather, the movements of the sea animals and of the ice are never exactly the same. Nature asks of you only attention and time.
The old Inuit concept of time sees no time spent, no time wasted, no time gone. Time arrives. Time only arrives. Each and every moment we receive the gift of time to be added to all the gifts of time already received. Yes, nature is cyclical, yet still unpredictable; the variations in weather, the movements of the sea animals and of the ice are never exactly the same. Nature asks of you only attention and time. change what all this means to me now. I have gained an insight that I would almost call spiritual, where even my ancestors and the story of my extended and immediate family belong. And where all of you (in this community) belong. Instead of disconnection there is now connection, over space and over time. There is, in each moment, attention, time and power to grow.
change what all this means to me now. I have gained an insight that I would almost call spiritual, where even my ancestors and the story of my extended and immediate family belong. And where all of you (in this community) belong. Instead of disconnection there is now connection, over space and over time. There is, in each moment, attention, time and power to grow.
 When I was 24 years old I went to the last of over a dozen treatment and detoxification centers I have attended. I was, and had always been, resistant to the 12-step approach to recovery, and I did not resonate with many of its underlying principles regarding the causes and treatment of addiction. But I followed the lead of some open-minded people at my last treatment center and began attending 12-step meetings voluntarily. And I began to recover. There is much that I learned from my 12-step involvement, the most important being the utilization of
When I was 24 years old I went to the last of over a dozen treatment and detoxification centers I have attended. I was, and had always been, resistant to the 12-step approach to recovery, and I did not resonate with many of its underlying principles regarding the causes and treatment of addiction. But I followed the lead of some open-minded people at my last treatment center and began attending 12-step meetings voluntarily. And I began to recover. There is much that I learned from my 12-step involvement, the most important being the utilization of  some kind of growth modality instead of simply trying to stop using. I also began identifying with others who had attachment wounds like mine, even if these concepts were not discussed overtly. I created some deep and lifelong friendships and learned about the fulfillment that comes from service to others. The Twelve Steps taught me that deep emotional change must be incrementally worked toward with diligence and sustained focus, and gave me a prescribed external structure (meetings,
some kind of growth modality instead of simply trying to stop using. I also began identifying with others who had attachment wounds like mine, even if these concepts were not discussed overtly. I created some deep and lifelong friendships and learned about the fulfillment that comes from service to others. The Twelve Steps taught me that deep emotional change must be incrementally worked toward with diligence and sustained focus, and gave me a prescribed external structure (meetings,  commitments, and step-work) upon which to start building these changes. Finally, in the beginning, it gave me a large group of people with whom I could openly share my struggles and successes, finally building a sense of personal competence and esteem.
commitments, and step-work) upon which to start building these changes. Finally, in the beginning, it gave me a large group of people with whom I could openly share my struggles and successes, finally building a sense of personal competence and esteem. by most members. I am also not remotely religious, and never attributed my ability to abstain to a higher power. Finally, and this became more apparent after I left 12-step involvement—especially after I incorporated moderate alcohol use into my life a few months later—listening to similar messages
by most members. I am also not remotely religious, and never attributed my ability to abstain to a higher power. Finally, and this became more apparent after I left 12-step involvement—especially after I incorporated moderate alcohol use into my life a few months later—listening to similar messages  repeatedly for years created a type of programming that made the idea of leaving difficult. To do so, I had to contend with deep feelings of fear caused by overt messages that leaving would inevitably lead to relapse and the loss of everything that I had spent so many years creating. Leaving also elicited deep feelings of shame and guilt that lasted acutely for months, and their tendrils still infect me two years later.
repeatedly for years created a type of programming that made the idea of leaving difficult. To do so, I had to contend with deep feelings of fear caused by overt messages that leaving would inevitably lead to relapse and the loss of everything that I had spent so many years creating. Leaving also elicited deep feelings of shame and guilt that lasted acutely for months, and their tendrils still infect me two years later. My addiction story is ruled by two deep, seemingly contradictory, truths: first, that deciding to become a 12-step member was one of the best decisions I’ve ever made. And second, that deciding to leave 12-step membership was one of the best decisions I’ve ever made. I wish that it weren’t anathema within the 12-step paradigm to leave either for periods or forever, but I kind of get it. I benefited from the same rigidity within 12-step doctrine that eventually repelled me. I may have temporarily needed that rigidity to counteract the evermore rigid attachment I had to heroin. I needed the external structure offered by the 12-step program and traditional abstinence until I could incorporate my own version of structure, inwardly. I needed form until I could safely find formlessness.
My addiction story is ruled by two deep, seemingly contradictory, truths: first, that deciding to become a 12-step member was one of the best decisions I’ve ever made. And second, that deciding to leave 12-step membership was one of the best decisions I’ve ever made. I wish that it weren’t anathema within the 12-step paradigm to leave either for periods or forever, but I kind of get it. I benefited from the same rigidity within 12-step doctrine that eventually repelled me. I may have temporarily needed that rigidity to counteract the evermore rigid attachment I had to heroin. I needed the external structure offered by the 12-step program and traditional abstinence until I could incorporate my own version of structure, inwardly. I needed form until I could safely find formlessness.
 Hanna is one of several addiction researchers who wrote commentaries about my book and my theory of addiction. Here she explains how we can view addiction as guided by choice without the extra baggage of blame, shame, and stigma. Following are segments of her revised commentary,
Hanna is one of several addiction researchers who wrote commentaries about my book and my theory of addiction. Here she explains how we can view addiction as guided by choice without the extra baggage of blame, shame, and stigma. Following are segments of her revised commentary,  bad character with antisocial values: selfish and lazy, they supposedly value pleasure, idleness and escape above all else, and are willing to pursue these at any cost to themselves or others. In contemporary Western culture, we typically hold people responsible for actions if they have a choice and so could do otherwise, and we excuse people from responsibility if they don’t. Because the moral model of addiction sees drug use as a choice, it views addicts as responsible — deserving of the stigma and harsh treatment they in fact receive.
bad character with antisocial values: selfish and lazy, they supposedly value pleasure, idleness and escape above all else, and are willing to pursue these at any cost to themselves or others. In contemporary Western culture, we typically hold people responsible for actions if they have a choice and so could do otherwise, and we excuse people from responsibility if they don’t. Because the moral model of addiction sees drug use as a choice, it views addicts as responsible — deserving of the stigma and harsh treatment they in fact receive. For those who recoil from the attitudes embodied in the moral model, the disease model of addiction can appear by contrast to offer a desperately needed [alternative]. “When addiction specialists say that addiction is a disease, they mean that drug use has become involuntary.” According to the disease model, addiction is a chronic, relapsing neurobiological disease characterised by compulsive use despite negative consequences. Repeated drug use is supposed to change the brain so as to render the desire for drugs irresistible: the disease model maintains that addicts literally cannot help using drugs and have no choice over consumption.
For those who recoil from the attitudes embodied in the moral model, the disease model of addiction can appear by contrast to offer a desperately needed [alternative]. “When addiction specialists say that addiction is a disease, they mean that drug use has become involuntary.” According to the disease model, addiction is a chronic, relapsing neurobiological disease characterised by compulsive use despite negative consequences. Repeated drug use is supposed to change the brain so as to render the desire for drugs irresistible: the disease model maintains that addicts literally cannot help using drugs and have no choice over consumption. Experimental studies show that, when offered a choice between taking drugs or receiving money then and there in the laboratory setting, addicts will frequently choose money over drugs. Finally, since Bruce Alexander’s seminal experiment “Rat Park” first intimated that something similar might be true of rats, animal research on addiction has convincingly demonstrated that…cocaine-addicted rats will…forego cocaine and choose alternative goods, such as saccharin or same-sex snuggling, if available. In short, the evidence is strong that drug use in addiction is not involuntary: addicts are responsive to incentives and so have choice and a degree of control over their consumption in a great many circumstances.
Experimental studies show that, when offered a choice between taking drugs or receiving money then and there in the laboratory setting, addicts will frequently choose money over drugs. Finally, since Bruce Alexander’s seminal experiment “Rat Park” first intimated that something similar might be true of rats, animal research on addiction has convincingly demonstrated that…cocaine-addicted rats will…forego cocaine and choose alternative goods, such as saccharin or same-sex snuggling, if available. In short, the evidence is strong that drug use in addiction is not involuntary: addicts are responsive to incentives and so have choice and a degree of control over their consumption in a great many circumstances. The second reason to maintain a choice model of addiction is that the process of overcoming addiction through a sense of agency, empowerment, and personal growth and self-understanding — a process that Lewis describes in The Biology of Desire with great care and acuity — itself presupposes that addicts have choice and a degree of control. Agency needs to exist to be mobilized: you can only decide to quit and do what it takes to stop using and change how you live and the kind of person you are if you have some choice and control over your use and your identity.
The second reason to maintain a choice model of addiction is that the process of overcoming addiction through a sense of agency, empowerment, and personal growth and self-understanding — a process that Lewis describes in The Biology of Desire with great care and acuity — itself presupposes that addicts have choice and a degree of control. Agency needs to exist to be mobilized: you can only decide to quit and do what it takes to stop using and change how you live and the kind of person you are if you have some choice and control over your use and your identity. sensory curiosity – expanded experiential horizon; and, finally, (7) euphoria and hedonia – in other words, pleasure. Drugs make us feel good, provide relief from suffering, and help us do various things we want to do better. [It] is difficult to see what could possibly be wrong with using drugs in and of itself. Suppose now we ask a further direct question: When use escalates to the point of addiction, who is to be held responsible for the ensuing negative consequences? According to the moral model, it is addicts themselves, who are not only responsible but [blameworthy], as they are considered to be fundamentally people of bad character with antisocial values… As an advocate of a choice model of addiction, I do not of course deny that some responsibility — but, crucially, responsibility as distinct from blame — lies with addicts themselves… The point I wish to emphasise however is that, in placing blame squarely on addicts or their disease, both models are united in enabling us to keep the focus of our attention away from ourselves and our society, avoiding the question of whether we, as a society, also collectively bear some responsibility for drug use and addiction and their consequent harms.
sensory curiosity – expanded experiential horizon; and, finally, (7) euphoria and hedonia – in other words, pleasure. Drugs make us feel good, provide relief from suffering, and help us do various things we want to do better. [It] is difficult to see what could possibly be wrong with using drugs in and of itself. Suppose now we ask a further direct question: When use escalates to the point of addiction, who is to be held responsible for the ensuing negative consequences? According to the moral model, it is addicts themselves, who are not only responsible but [blameworthy], as they are considered to be fundamentally people of bad character with antisocial values… As an advocate of a choice model of addiction, I do not of course deny that some responsibility — but, crucially, responsibility as distinct from blame — lies with addicts themselves… The point I wish to emphasise however is that, in placing blame squarely on addicts or their disease, both models are united in enabling us to keep the focus of our attention away from ourselves and our society, avoiding the question of whether we, as a society, also collectively bear some responsibility for drug use and addiction and their consequent harms. struggle with mental health problems, and are members of minority ethnic groups or other groups subjected to prejudice and discrimination. They may experience extreme psychological distress alongside a host of mental health problems apart from their addiction, feel a lack of psychosocial integration, and are at a socioeconomic disadvantage such that they have severely limited
struggle with mental health problems, and are members of minority ethnic groups or other groups subjected to prejudice and discrimination. They may experience extreme psychological distress alongside a host of mental health problems apart from their addiction, feel a lack of psychosocial integration, and are at a socioeconomic disadvantage such that they have severely limited  opportunities. These circumstances are central to understanding addiction in many contexts. Put crudely, the reason is simply that drugs offer a way of coping with stress, pain, and some of the worst of life’s miseries, when there is little possibility for genuine hope or improvement… In such circumstances, whatever harms accrue from using drugs must be weighed against whatever harms accrue from not using them. For this reason, the explanation of addiction and its associated negative consequences must lie in no small part with the psycho-socio-economic circumstances that cause such suffering and limit opportunities. And the existence of these circumstances is a feature of our society for which we must all collectively take some responsibility.
opportunities. These circumstances are central to understanding addiction in many contexts. Put crudely, the reason is simply that drugs offer a way of coping with stress, pain, and some of the worst of life’s miseries, when there is little possibility for genuine hope or improvement… In such circumstances, whatever harms accrue from using drugs must be weighed against whatever harms accrue from not using them. For this reason, the explanation of addiction and its associated negative consequences must lie in no small part with the psycho-socio-economic circumstances that cause such suffering and limit opportunities. And the existence of these circumstances is a feature of our society for which we must all collectively take some responsibility.
 too religious, dogmatic, disempowering, cultish. Which is unfortunate because although 12-step is not the only way to get sober, it is one way, and it’s been effective for millions of people over the past 80 years.
too religious, dogmatic, disempowering, cultish. Which is unfortunate because although 12-step is not the only way to get sober, it is one way, and it’s been effective for millions of people over the past 80 years. In recent years I’ve been studying neuroplasticity on an informal basis and applying its principles to my daily life, especially vis-à-vis my addictive propensities: Chocolate truffles! Mad Men! Facebook!
In recent years I’ve been studying neuroplasticity on an informal basis and applying its principles to my daily life, especially vis-à-vis my addictive propensities: Chocolate truffles! Mad Men! Facebook! strengthens your capacity to do so again. Thanks to your malleable brain, the more you do something sober the easier it becomes. But you may need to muddle through a thousand situations sober before it comes as naturally as it did when you were drunk. It’s hard for most of us to stick to our resolve that many times. But with the support of others it is possible.
strengthens your capacity to do so again. Thanks to your malleable brain, the more you do something sober the easier it becomes. But you may need to muddle through a thousand situations sober before it comes as naturally as it did when you were drunk. It’s hard for most of us to stick to our resolve that many times. But with the support of others it is possible. AA contends that because our willpower has “failed utterly” to get us sober, we have no recourse but God. Really? Well, what does every participant at every meeting find every time? What is the common denominator? Not God, but other people getting sober. We find community. The generous support of other human beings carries us when we cannot carry ourselves.
AA contends that because our willpower has “failed utterly” to get us sober, we have no recourse but God. Really? Well, what does every participant at every meeting find every time? What is the common denominator? Not God, but other people getting sober. We find community. The generous support of other human beings carries us when we cannot carry ourselves.