
I just listened to the first 15 minutes of a lecture by Robert Sapolsky, a renowned biologist and Stanford professor. Sapolsky begins with an incisive lesson on why humans rely on categories. Categories, he says, make it easier to think about complex phenomena. And human social behaviour is nothing if not complex. My friend Tom insisted that this online lecture series was worth viewing, and he’s right. I plan to view the rest. But first, this post.
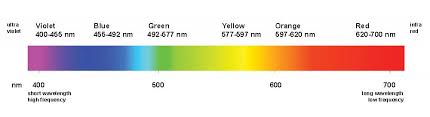
Take something a little simpler than human behaviour. If a colour falls between orange and yellow, you’ll have a harder time thinking about that colour and remembering it than if it’s either orange or yellow. Yet light frequencies fall along a continuum without boundaries. In other words, we actually invent colour boundaries, and different cultures see colour differently. It’s easier to remember a shape if you can call it a circle or a square than if it doesn’t fit any geometrical category. If the shape is squarish with rounded corners, or blob-like, you’ll have a harder time thinking about it, remembering it, and using it in a conceptual task. (Sapolsky demonstrates these examples on the white board.)
So, okay, categories are tools for simplifying perception and thought. But there are several down sides to categorical thinking. Sapolsky mentions a few, but here’s the one that inspired this post. Remember when 65 was  the cut-off between a pass and a fail? (That was the cut point when I was an undergrad.) So you’ve spent much of the week partying, getting high, etc, and here comes the exam, and you cram for it that morning, give it your best shot, and wait anxiously for the result. A
the cut-off between a pass and a fail? (That was the cut point when I was an undergrad.) So you’ve spent much of the week partying, getting high, etc, and here comes the exam, and you cram for it that morning, give it your best shot, and wait anxiously for the result. A  week later the prof hands out the exams, or you look up your grade on the bulletin board, and the thing you care about more than anything else is whether you got at least a 65. If you got a 64, you’re shit out of luck. If you got a 66, you’re sailing.
week later the prof hands out the exams, or you look up your grade on the bulletin board, and the thing you care about more than anything else is whether you got at least a 65. If you got a 64, you’re shit out of luck. If you got a 66, you’re sailing.
Now how much difference is there, really, between a 64 and a 66? How much information does that distinction actually give you, about your performance, your dedication, your intelligence, or your use of free time?
This isn’t the first time I’ve conceptualized addiction (intensity, duration, riskiness, etc) as a continuum — a continuum that does not lend itself at all to two categories, disease vs. health. Other addiction thinkers, researchers, treatment providers, etc, have also remarked that addiction  is a spectrum, a dimension, a set of gradations at best — nothing like an all-or-nothing category. Yet the disease label cannot help but classify addiction as a category. You either have tuberculosis, or diabetes, or cancer, or you don’t. Never mind that, when it comes to addiction, the category label itself can do more harm than good. As soon as you classify addiction as a disease, you draw a line. (There is some discussion of this issue in the commentaries on an article of mine.)
is a spectrum, a dimension, a set of gradations at best — nothing like an all-or-nothing category. Yet the disease label cannot help but classify addiction as a category. You either have tuberculosis, or diabetes, or cancer, or you don’t. Never mind that, when it comes to addiction, the category label itself can do more harm than good. As soon as you classify addiction as a disease, you draw a line. (There is some discussion of this issue in the commentaries on an article of mine.)
Indeed, the disease labelling trend in the US and elsewhere makes it stupidly easy to put addiction in a wastebasket category. You’ve either got it or you don’t. And if you’ve got it, then free choice, self-control, empowerment, and so many other features of human thought and emotion are neatly defined. Easier to think about, right?

Sapolsky makes other cool points about how categorical thinking obscures real complexity. For example, falling into the same category doesn’t necessarily mean that two things are similar. As we know, two people, both categorized as having the disease of addiction, can be as different as giraffes and field mice (just two animals that came to mind).
Many of my readers will probably agree that categorical thinking, this mental-labour-saving device, misses so much — so much of the real complexity of addiction — that it can’t help but muddy the waters.
………………………..
This is remarkable: four hours after posting today’s post, I found an email in my inbox that contained nothing more than this link. If this man can face his addiction and challenge it, without submitting to the disease categorization, then…that’s all there is to say. The post is electrifying, extremely well written, and deeply moving. I’m honoured that my work figures in his thinking.
Leave a Reply