
I got back Saturday from a 3-week extravaganza: first the Nobel conference on Addiction, then two weeks as a visiting prof at Gustavus College, and then a week in Toronto, catching up with relatives and friends, hanging out with my daughter, and doing about one talk per day on…you know, addiction not being a disease, that sort of thing. We’ve got a lot to catch up on.
 Let’s start with the conference. The Nobel Foundation (yes, the big guys, and no, I did not get a prize — they’re often awarded posthumously so I should be grateful) has been hosting this annual event at Gustavus Adolphus College. I’d never heard of it either, but it’s a high-ranking liberal arts college near Minneapolis. This year “addiction” was the topic. So I was pleased to be invited and especially glad that I’d be meeting Carl Hart.
Let’s start with the conference. The Nobel Foundation (yes, the big guys, and no, I did not get a prize — they’re often awarded posthumously so I should be grateful) has been hosting this annual event at Gustavus Adolphus College. I’d never heard of it either, but it’s a high-ranking liberal arts college near Minneapolis. This year “addiction” was the topic. So I was pleased to be invited and especially glad that I’d be meeting Carl Hart.
 He was easily the most dashing speaker at the conference — a tallish, slim black man with long dreads, handsome, friendly, cool, and collected. His book, High Price, is one of the most popular books on addiction of the past few years. Carl’s talk came on day 2 of the conference, and the crowd of 4,000 present (and supposedly another 10,000 online) were ready for some meat. Yesterday’s talks had generally tiptoed around what many considered the main issues.
He was easily the most dashing speaker at the conference — a tallish, slim black man with long dreads, handsome, friendly, cool, and collected. His book, High Price, is one of the most popular books on addiction of the past few years. Carl’s talk came on day 2 of the conference, and the crowd of 4,000 present (and supposedly another 10,000 online) were ready for some meat. Yesterday’s talks had generally tiptoed around what many considered the main issues.
So he gets up in front of an audience of rosy-cheeked, blonde midwesterners and proclaims that 80 – 90% of recreational drug users are not addicts and never will be. And most people who use drugs don’t need jail and they don’t need medical treatment. Even the addicts — especially the addicts — are the last people one would ever want to put in prison. Massive applause. The most important thing we can do for drug users, young or old, is to educate them. Just like with sex and driving — other activities that are potentially fun and potentially harmful — users need to know how to stay safe. The crowd likes this guy, and so do I. There’s laughter and applause. It makes sense.
He provided an example of drug education specifically targeted to this audience: when you eat cannabis it takes a long time to feel the effects. So don’t keep eating brownies until you know how strong they are! More laughter, more applause, some clearing of throats from the elders. Everyone is transfixed. Hart is deliberately opening a rift between the beliefs and sensibilities of young people who are presumably experimenting with drugs and the stodgy older generation who are starting to fidget in their seats. Fascinating to watch.
 But things got a bit weird when he got onto methamphetamine. He showed some footage designed to scare people away from meth: a clip of a man writhing on the floor as though possessed by demons. He said he could not even imagine what symptoms this man was expressing — in other words, he was ridiculing the kind of “drug education” that has become status quo in the U.S. Good point. But then he went on for a long time about meth being chemically similar to Adderall, a stimulant used for ADHD. He showed slides of two molecules that looked the same except for a methyl group and apologized for speaking over the heads of the less scientifically inclined. I thought that was a cheap trick. I wasn’t convinced that Hart knew much about methyl groups to begin
But things got a bit weird when he got onto methamphetamine. He showed some footage designed to scare people away from meth: a clip of a man writhing on the floor as though possessed by demons. He said he could not even imagine what symptoms this man was expressing — in other words, he was ridiculing the kind of “drug education” that has become status quo in the U.S. Good point. But then he went on for a long time about meth being chemically similar to Adderall, a stimulant used for ADHD. He showed slides of two molecules that looked the same except for a methyl group and apologized for speaking over the heads of the less scientifically inclined. I thought that was a cheap trick. I wasn’t convinced that Hart knew much about methyl groups to begin 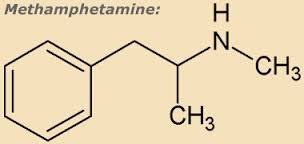 with. He’s a psychologist, not a chemist. In fact, methamphetamine is not the same as Adderall, which is a mixture of dextroamphetamine and levoamphetamine. Meth is far more powerful, especially given its conventional modes of ingestion, and far more addictive. So what was the message here?
with. He’s a psychologist, not a chemist. In fact, methamphetamine is not the same as Adderall, which is a mixture of dextroamphetamine and levoamphetamine. Meth is far more powerful, especially given its conventional modes of ingestion, and far more addictive. So what was the message here?
I’d read Hart’s book, cover to cover, in the month preceding the conference. What made him famous was his research program, conducted at Columbia University, showing that crack and meth addicts didn’t have to lunge for a hit of dope every time it became available, if they had other choices. He kept self-identified addicts in a residential setting for three weeks at a time, and he gave them choices between monetary (or other) rewards and various-sized hits of crack or meth. And since they didn’t get the money until they left the residence, they couldn’t go out and spend it on the street. Sure enough, meth and crack addicts often chose the money instead of the drug, especially when the money offered was at the high end of the scale and/or the dosage was at the low end. According to Hart, this demonstrated that addiction is a choice, not a disease. Addicts don’t lose their free will, as Nora Volkow might insist. They can make choices when choices are available.
I really like Hart’s argument in one respect. He is trying to show that inner-city kids who don’t have much to do except take drugs are more likely to take drugs — as a choice, not a compulsion. And I fully concur with his message about the disadvantages faced by minority members, both when it comes to choosing drugs and when it comes to the vastly disproportionate jail sentences they’re hit with — because of the built-in racial bias in laws that, for example, punish the use of crack (a “black drug”) 20 – 50 times more harshly than the use of powder cocaine (a “white drug”) despite their chemical similarity. Johann Hari gave us the same message, loud and clear. And it needs to be heard.
But I find other aspects of his message highly questionable.
First, does anyone, even Nora the Terrible, really believe that addicts cannot control their addictive impulses, even for a little while? I doubt it. That seems like a classic straw-man argument. It’s an  exaggerated claim, so it’s not that hard to rebut. Second, how much crack or meth is he offering these guys? The dosage information is in the book and related papers, but if you are offering crack or meth addicts smallish doses many times a day, day after day, surely their tolerance will soon override the potential high. Mightn’t the drug offer become just a tease? Hart doesn’t seem to care about these issues. He does not use self-report to evaluate the level of the high. And he doesn’t show how the choices might change over time (within the residency period), potentially reflecting a day-by-day build-up of tolerance.
exaggerated claim, so it’s not that hard to rebut. Second, how much crack or meth is he offering these guys? The dosage information is in the book and related papers, but if you are offering crack or meth addicts smallish doses many times a day, day after day, surely their tolerance will soon override the potential high. Mightn’t the drug offer become just a tease? Hart doesn’t seem to care about these issues. He does not use self-report to evaluate the level of the high. And he doesn’t show how the choices might change over time (within the residency period), potentially reflecting a day-by-day build-up of tolerance.
Carl Hart got the only standing ovation of any of the speakers. Hooting, whistling, on-your-feet cheering coursed around the auditorium for several minutes. Especially from the young people — the undergrads and high school students. Indeed his message was powerful, both courageous and outrageous: the middle-class, middle-of-the-road masses (young and old, expert and novice) needed to be confronted with the distortions, in fact the lies, that have been beamed at us through every conceivable media channel from the overlords of the War on Drugs.
I liked this Carl Hart. I stood up and applauded with the rest. But I wanted there to be another Carl Hart as well: one who addressed the 10 – 20%, the ones who suffer, the addicts.
When someone from the audience asked him what he would say to his kid, if the kid told him he was thinking of trying meth, Hart said he would try to educate the kid about how to stay safe, whatever drug he was taking. That’s not the answer I would have given. I would have said: smoke weed, try mushrooms, and here are some tips about doing it safely. But stay away from meth.
Comments
60 responses to “Hart to Hart: drug use, race, and addiction”
You mean the sad. The sad for what ever reason make up the large proportion of so called addicts. There are many reasons to be sad and few teachers on how to be glad. Carl offered a glad. and it is that simple. Why have we made this so hard. The majority of those but behind bars are those that are blacks or sad. Disease was never the problem. But this society needed something to point. The symptom of that has always been black or lacking and sad. The issue has always been about the advantaged vs. the disadvantaged and Carl points that out. For certain, it is no real documented “disease” just a dis-ease which apparently this society chooses to ignore. Not a good move.
working with Aboriginal men I observe that many use drugs and alcohol because their lives are empty – but there is a point of no return – where habits become addictions – where as Lewis says impulsiveness is replaced by compulsiveness. I know the compulsiveness of severe alcoholism – there is little choice involved – keep drinking or be very ill in withdrawal – they become not great options to choose from
That’s right. There is still choice involved but it becomes squeezed into a corner by the power of the compulsion.
This guy Carl is so spot on! It has nothing to do with the drug or alcohol~!!!!!!! Why do we as a society defer to that rather than asking the person what the problem is ?
Marc, you as a Nuro scientist have always confirmed this. I am only attracted to both you and Carl because as a manager of sober houses for 4 years it became obvious to me. And my angst has been dealing with a society that wants to treat the symptoms of a disorder rather that addressing the base disorder. The base disorder covers a wide rage from ignorance to depression.
And I would add to hormonal which few have addressed or researched.
Thanks for this post. it is one of the last few that have made sense to me.
You’re welcome!
The young girls in my sober houses were near completing collage and still having no idea what they were going to do. The older women who were post and pre menopausal had their own set of circumstances which go from desired sex drive to empty nest syndrome. No one is addressing the hormone factor!!!! It exist, it is real and it has symptoms which are not always addressed in the best way.
“First, does anyone, even Nora the Terrible, really believe that addicts cannot control their addictive impulses, even for a little while?”
Aside from the dig to the NIDA director, I agree with this critique of Dr. Hart’s claims. There is a difference between the behavior of drug use and being dependence upon the drug. The latter doesn’t simply disappear given a better choice (e.g., money). At some point, no amount of monetary reward may be sufficient to overcome the cravings and withdrawal from their drug. Three weeks is not a long period of time, and its unclear what happens after the experiment is done. Likely, the subjects in the study are smart enough (i.e., street wise) to know the comparative value of the money the study’s offering them vs. the value of the drug Hart’s offering them. Hart’s logic is also flawed: I suppose one could be offered increasingly large sums of money to not eat food for three weeks, so to some extent eating is a “choice”, but at some point, biological (and psychological) processes will strongly demand that you eat. Drug addicts’ biological and psychological imperative to use drugs is not as dire as this analogy, but it suggests there is something more going on than drug use being just about free will.
The dig was meant with a bit of tongue in cheek. Many of those who take a social/behavioral rather then medical approach to addiction tend to villainize her. I know that she is a sincere person and a great scientist.
I think your idea of a food reward as a control (or at least comparative) condition is fabulous. There are a lot of ways we could untangle what goes on in those three weeks, but that’s not what Hart wants to do. He wants to make the point that addictive behavior is chosen, not compelled…..and that’s about all he wants to show. I hope he will go on to refine the experimental design. There’s a lot we can learn in this paradigm.
If you want a refinement on Hart’s process, look to Contingency Management: a well-known experimental treatment paradigm that has used money, vouchers, and prizes as an alternative reinforcers to deter drug use. In the beginning, Stitzer used money but soon abandoned it as a reinforcer probably due to something like what Brain mentioned in his comment. Vouchers (used to purchase merchandise tailored to someone’s treatment plan) were used in the Higgins et al., 1994 experiment, and then CM took off. Unfortunately it’s still not widely available in the treatment world. CM works for meth, cocaine, MJ, alcohol, opiates, and nicotine. It was founded on behavioral economics and thought to work as a positive reinforcer for the non-drug use behavior, but the numbers don’t quite work, especially considering pre-clinical studies (e.g., Woolverton). Either high drug costs or high alternative rewards are needed to deter drug use. CM doesn’t use that high value of a reward, especially in the beginning (worth of vouchers accumulate and increase with increased abstinence – over months). My old advisor, David Redish, and I hypothesized that it works by offsetting more automatic processes by engaging the deliberative system (http://www.ncbi.nlm.nih.gov/pmc/articles/PMC4450586/) but only for some people. Brian is probably right. There comes a point where no amount of reward or alternative choice will detract an individual with addiction from using, due to severely compromised neurobiology.
I think that what Hart is doing is really important for the disadvantaged community, and what Volkow is doing is really important for the addiction research community (and frankly the addiction community in general – by reducing stigma).
Is there a way in which we might draw on each other’s strengths?
Best,
Paul
Hi Paul. For sure we should draw on each other’s strengths. By pointing out weaknesses in the arguments of some of the different camps, I don’t mean to negate their contributions. Nora Volkow’s research has been enormously useful. But I don’t believe that the destigmatization supposedly provided by the disease label offsets the disadvantages…especially, the fatalism inherent in the notion of a chronic brain disease. As for Carl Hart, I was clear about what I like — and what I find lacking.
Thanks for your review of contingency management. I don’t know the research well, but I know that’s it’s been shown to be effective. Here in the Netherlands people are working on approach-avoid training — for example teaching alcoholics to use a joystick to push away (rather than pull toward) images of alcohol. These automatic / unconscious processes may be what are working against the deliberative system you point to in CM. Or….CM may work at an unconscious as well as a conscious level, changing biases in attention and response.
Anyway, we surely do have a lot to learn from each of the different research paradigms.
The paradigm that addictive behavior is chosen, not compelled,
can be corroborated, and probably by many of the people that read this blog.
At some point, the realization that you are making a conscious, deliberate decision, and are undertaking a physical action to ingest or engage with the addictive behavior, can occur during the recovery process.
This is quite different to the popular analogy which likens addiction and recovery to walking down a road, and avoiding falling down a hole.
The realization that you have to consciously seek out, and then climb the lip of the hole in the road to enter it, can be life-changing.
Discovering that recurring inebriation or use is not accidental, and also requires you own specific effort, is a re-discovery of freedom that had been eclipsed during the addiction.
Carl Harts experimental design helps crack the mold of the disease-mindset, but the focus has rarely been on the nascent phenomena of recovery.
It seems logical and promising that key insights into addiction and the recovery process will be found there.
I agree with the gist of your message, Carlton, but there is such a thing as compulsion. Automatic behaviour has been studied since at least the time of Pavlov. What I”m after is a framework that encompasses both of the choice perspective (which you describe so well) and the dark workings of the mind-brain, which we can get to through psychology, neuroscience and other routes as well. Choice doesn’t vanish in the face of compulsion (when your dorsal striatum is firing in the red zone) but it sure becomes more difficult to choose one of the two options.
My apologies again-
“not just compelled” was intended in the first line.
Carlton,
“The realization that you have to consciously seek out, and then climb the lip of the hole in the road to enter it, can be life-changing.
Discovering that recurring inebriation or use is not accidental, and also requires you own specific effort, is a re-discovery of freedom that had been eclipsed during the addiction.”
That is an excellent description of the process. Said much better than I could probably describe it. Thanks for sharing that. I feel like it is exactly the process I went through. On the other hand, I am still a bit confused as to how I finally figured it out. :))
Mark P.,
Glad this comes across, and for the lack of a better term, the “Common-Sence-Ness” about many things becomes naturally apparent again if the compulsive feelings change.
Here is another example of popular beliefs;
“you easily forget”,and “you must keep reminding yourself” are life-long assumptions about addiction.
These types of beliefs serve as helpful, community-binding beliefs, particularly if you embrace and find the Disease model comforting.
But when the blinding, tunnelvision-generating compulsive feelings of an addiction alter or change, (as some readers have described in “Beginner’s Mind and Recovery”, It can naturally become apparent that a person does not to need to keep reminding themselves about things.
For example:
Say you are a major fan of a bands music..you buy tickets, go to all the concerts, etc, etc.
If your feelings for the music changes, you don’t have to keep reminding yourself NOT to purchase tickets and go to the concerts.
Thanks for this Carlton. There is something we’re missing when changing behavior, but not attitude in addiction. Is there a “best” way to do this?
It seems that when the feelings that the addiction is like a haven… changes to feelings that you are imprisoned by the addiction, the behavior naturally changes.
But “attitude” is really an individual thing,
I don’t think the can be a “best or even “worst” attitude.. it is such an individual thing.
Maybe I’m not sure what you mean by attitude being such an individual thing. Yes, it’s individual, but it’s a collocation of feelings and mental events that form a person’s perspective or philosophical bent. People’s feelings and behaviors change all the time but attitudes, although mutable, are relatively stable. They’re the lens through which we navigate and interpret the world– and our feelings about it. I would argue that whether I feel the addictive behavior is a “haven” or an “imprisonment” is an attitude, or a perspective at a meta-level above feelings or behaviors. I may feel nostalgic, or rattled or like I could use a pharmaceutical bump, but my attitude has shifted. I know if I reach for that shiny object I’m consciously and purposefully reaching for everything I know comes along with it. I know that’s not what I want. I may be getting picayune here but I think that’s an attitude– superordinate to thoughts, feelings and behaviors.
That is well described, and perhaps its the word “best” is what I dont feel comfortable with about answering here..
In a discovery-based idea of recovery, only the individual that discovers things that are best or worst, etc..
Marc, you wrote: “Hart is deliberately opening a rift between the beliefs and sensibilities of young people who are presumably experimenting with drugs and the stodgy older generation who are starting to fidget in their seats.”
Curious if you could talk more about this….do you see this as a valuable new element opening up new territories of perception or awareness for addicts and the public at large?
I see it as valuable, Carlton. That’s why I joined the standing ovation. Hart’s message needs to get out there and, yes, it will pull those with open minds further from the prevalent view that drugs are evil, users are sick, and those who won’t tow the line should be in jail. The young are always where new perspectives propagate, right? Not the old fogies. Especially the old fogies in middle America, if you’ll forgive me my biases.
I just think he ignores something really important about drug use: serious addiction. In fact I think he sweeps it under the rug to highlight what he believes to be a more important point.
Yes, I Agree.
Many of the old terms of previous Mindsets may become eclipsed with new, more applicable ones, based on the insights now occurring.
Terms like “Coming Clean” , “Growing up”, “Hitting bottom”, and others, come from another age and mindset, and can distract and congest progress in the understanding of Addiction and…. Recovery, (which is an old term from another mindset in itself 🙂
This was interesting to me, as so many things are these days, as a perspective on how my experience as a young person is becoming more remote as the distance from it in time increases. The discussion reminded me of a saying that was popular back in the day: Would you rather live in a time of money and no dope, or dope and no money? The answer was, of course, the latter, because what the hell did we need money for if there was no dope (read that, grass/pot/weed) to buy. Which leads back to Mark’s final comment which is really important: any serious discussion about drugs/addiction has to differentiate which drugs are being talked about. The experience of addiction is different qualitatively for different drugs, and should be considered when studying and/or treating the addictions.
Hi Denise. Exactly. Differences in substances are a critical part of the discussion. Gene Heyman shows radically different developmental curves for the time it takes to get off different substances (on average). For example, with cocaine he shows a median of 4 years to quit….for alcohol I think it’s 15 years or so. These averages are slippery, but they’re one way to show how different different drugs are.
As for that saying about drugs and money, I remember it well: Fabulous Furry Freak Brothers, circa 1968. Thanks for the reminiscences!
Marc, you are my primary source of information on the neuro-science of addiction. It has become a joke to say that “I’m not a scientist” but I must confess it. I don’t follow all the arguments in your new book and I don’t have the time or inclination to verify it all. So I have to trust someone and I choose you as my authority.
On the other hand, I responded positively to what Carl Hart was saying in “The House I live In”. You say his basic study on the choices addicts are capable of making is fatally flawed. No argument here, I am not qualified to say.
But my main concerns around addiction are where the rubber meets the road through legal policy and popular attitudes. In the USA, where I live, but was not born, the politics are tortured and the matter of race is inescapable. Maybe Hart’s work is more sociology than neuro science?
Also, he is bound to have wider acceptance on a US University campus than an old white man like you (or me). It never hurts to look like a young Denzel Washington. It’s almost impossible to have any street cred once you admit to coming from Toronto, something I know from sad experience!
Very funny, Jeff. I got street cred from having been an addict, not coming from Toronto. And I’ll have you know that Hart was NEVER an addict. So there.
I didn’t mind that he got a standing ovation and I didn’t. Honest. In fact my talk was at the final banquet….maybe they would have stood if not encumbered by table legs. Though I doubt it. Look, I agree that the main message is really important. Johann Hari presented a very similar message in Chasing the Scream — in what I thought was a more compelling way. But never mind that. The times they are a changin’ and unique voices are coming together.
I think you hit the nail on the head when you say that Hart’s contribution is mainly in the realm of sociology. I cried when I read Hari’s description of the Tent City prisons for drug users in Arizona. Hari led me to this: http://www.mcso.org/JailInformation/TentCity.aspx I simply couldn’t believe his description of how bad things were until I googled his sources. The sociological message is critical. The situation is tragic.
Hello marc,
Im currently an undergraduate psychology student at memorial university currently studying the effects of drugs on the brain. I am very interested in your blog and i am a huge fan of your books! I think your take on carls speech is very similar to what mine would have been. Yes methamphetamine has a very similar structure to whats contained in adderall but methamphetamine and Adderall have very different effects and should not be compared in that way because of the huge difference. I also think it entirely depends on the dose as well. I also think some drugs are very hard to be taken safely and i agree with you there as well. You can toy around with marijuana and hallucinogens without getting addicted right away but i think meth is a whole different story!
HI Jamie. I’m glad we agree. Also see Denise’s message and my reply above. Cheers.
I remember a period of abstinence, some weeks in duration, and I recall it being a time of profound addiction. I had an ounce of crack stashed, within arms reach, but my intention was to save it for a future event, a binge in a hotel, at which to be confected with other addictive behaviours. So I saved it, craving it, and then went crazy (and the ounce proved to be much less than enough).
According to Carl Hart I wasn’t addicted, right? Because I had a choice (I most certainly did not). What’s interesting about the ten or twenty percent of us who use and can’t stop is not their we’re different. It’s that we’re like everybody else. We’re all creatures of habit, and we all do things that cause harm, for selfish reasons. Because were deluded in thinking we’re separate from each other–the worse example of which is define some of us as addicts with a chronic brain disease. But the biggest mistake isn’t that, it’s that by writing off addictions we’re missing a huge opportunity to learn about how human beings can change. All of us. We’re changing all the time. Stoned or not, we have to learn how to pay attention. Now for me much better not stoned (by the way).
I heard Johann Hari interviewed when Chasing the Scream was launched. I was mesmerised. He really made me step back and re-think quite a few things. But one strange – or not so strange – outcome was that the next time I was offered a joint (which doesn’t happen very often in my lifestyle) I imbibed … and enjoyed it. A shift had occurred and I had given myself permission to do something I had avoided skillfully for decades.
While I agree that Hart is raising an interesting debate and reaches deep into the paranoia much of the middle-class public have around the use of drugs, that lack of social acceptance does function as a useful a barrier to many individuals choosing not to use drugs. Should that barrier be lifted … wow. It’s a frightening prospect. While I concede that drug use would go up probably by many who choose to use drugs responsibly, there would also be a marked increase in suffering. At the end of the day, doesn’t ‘availability’ play a significant role in the development of drug dependence.
I don’t know what the answer is but it is a topic well worth robust public debate.
Hi Margot, The issue of decriminalization/legalization vs increased availability was also raised several posts ago, as triggered by Johann Hari’s book and the counterargument raised by Percy Menzies. I’m not so sure you’re right, that lifting the social barriers will increase addiction even if it does increase use. My understanding is that addiction went down — considerably — when Portugal decriminalized all drugs. Mind you, they spent the money saved by the court system on treatment for those who did have problems.
Many of us, perhaps most of us, have managed to develop robust addictions despite the social barriers we had to cross to get there. One thing accomplished by social rejection/social barriers is that people who do use drugs and become addicted feel an added burden of isolation and stigma.
Menzies argues that access leads to increased use. Maybe. But it does not necessarily lead to increased addiction. When Prohibition in the US was lifted in the late 30s, I think the wedge between addiction and use became much more conspicuous — and therefore easier to avoid.
Portugal gives us hope. I remember Johann talking about one law enforcement officer who looked back on his treatment of addicts with shame … such had been the shift in social consciousness.
Whether access leads to increased addiction is probably a question we won’t be able to answer unless we give it ago.
Lifting the social stigma would no doubt have greater ramifications than we can imagine. The reality is that the world is moving more and more toward performance enhancing drugs of one sort or another. It’s just that we’ve deemed some legal and some illegal. The idea of ending the war on drugs caused a shift in my openness to use drugs again but I’ve barely actually changed my behaviour and it certainly has not brought me any closer to a new addiction. I just found it interesting that it had this affect on me and was trying to extrapolate the potential repercussions in a more broader social sense. Great to encourage this debate.
Margot, you are a great example of what Johann and others say happens when the barriers are lifted: addiction does not go up. Because addiction is motivated by psychological pain and isolation…so why should it? In fact, almost nobody who feels comfortable in their own skin wants to become an addict. Access and openness have no impact on those self-imposed limits.
Marc, I love that you’ve raised this issue about Hart’s research. I really, really like the guy, too, and I think he adds much that is valuable to the conversation around drugs, but I’ve had the same sticking issue with the somewhat reductionist conclusions he draws from his research. Have you seen the article in The Atlantic called “The Science of Choice in Addiction”? It relies heavily on Hart’s research (I think the article came out shortly after his book was published) and heavily implies that “carrots and sticks” may be the way to go in “treating” addiction. I have issues with that, as well, because it seems to me that while incentives and consequences can be highly motivating for some, there is another contingent of addicted people for whom no amount of negative consequences seems to motivate positive change (often, quite the opposite) and a contingent who seemingly have every incentive to change (i.e., great family support, great job or other financial resources, etc.) who don’t. Would love your thoughts on that.
HI Gina. Sorry, I missed your comment until just now. No, I didn’t see that article, but I’ll look for it. Meanwhile, these two contingents you mention, the one unmoved by positives and the other unmoved by negatives…imply to me that the roots of addiction are really deep in the personality. Addiction grows as part of the personality, in my view, much like depression, suspicion of others, the sense of being wronged by the world.
I see addiction as a belief — a belief that taking something inside you will make you feel better. And of course beliefs are often much too resilient to be overturned by experience, data, logic, etc. And then there’s that third group for whom barriers increase the need and determination. I was like that when I was an addict. I would frequently say, fuck em, I’m going to do it anyway. Then climb through some second-storey window.
Given what we can see to be true for these three groups, I become less and less convinced that barriers, prohibition, and stigma have any value at all.
Interesting MRI experiment changing the brain of an addict …
http://video.pbs.org/video/2365597681/
David Eagleman’s PBS Special on The Brain
Mark, I would love to see this, but the Vimeo link you provided doesn’t work here….which is probably the same in the rest of Europe and maybe elsewhere. Can you give us the full title of the talk or the article?
Hi Marc,
Check with the European or Local PBS affiliate if there is one where you are.
It’s “The Brain with David Eagleman”
There are 6 sessions. The 4th has the MRI Experiment.
Here’s the PBS site listing all 6 …
http://video.pbs.org/program/brain-david-eagleman/
Best,
Mark
Everyone should give this a look!
I still can’t access the damn thing, but thanks for trying. I guess I’ll have to wait for my next visit to N America.
Can you summarize the findings in a couple of sentences? Or is there a journal article reference to the study? There should be if it’s legitimate research…
He basically dramaticizes a variety of different decision-making research, much of it in his Incognito book.
His addiction segment is basically a dramatization of this research:
http://sfn2013.conferencespot.org/55321-sn6-1.225941/t-001-1.227231/733-13-1.227272/733-13-1.227273
It looks to me like he’s trying to strengthen the impulse control circuitry by repeatedly triggering the urge to use and then successfully resisting it while the crack addict is in the scanner. Hopefully, it will then translate to the real world.
Thanks very much, Mark. I finally got a chance to go to this link…and it works fine for me…the Society for Neuroscience site. I’ll look at it now.
Much appreciated.
There is a level of analysis where every decision to use or not use is a choice, no matter how compelling and compulsive using seems. And the task of recovery coaches, sobriety buddies, drug counselors and support groups is to shift the default choice from using to not using. Get the person with the addiction to see it– that it’s possible. That it takes a lot of deep habit pattern unravelling, re-routing, or whatever the habit change process entails neurophysiologically– but it’s doable.
I was in a detox last week where the discussion moved to choice, it’s relativity and how the balance gets changed by the midbrain in addiction. There was a bright young man, who very sincerely asked, “But what if it isn’t about choice? It doesn’t feel like a choice to me. What do you do then?” He had a look of deep, pleading desperation on his face I’ll never forget. I did a little tap dance around habit change– it takes time, it’s a process you have to experiment with, and blah-be-dee-blah… Then his fellows in detox chimed in with support, solidarity and their own strategies. It helped him some, and bailed me out.
So I have a hypothetical question for the group. You’re in a detox, where a smart, sincere, dope-sick and desperate kid asks you this. What would you say to him? How do you reassure, enjoin pereverance, and give him hope? Give him a genuine pep talk?
What a great question, Matt. I have a few thoughts, which might include sneaking up on the thing….learning how to control use rather than “choose abstinence” which is so very difficult… But what do others think?
This is not a pep talk per se, but it may be a source of hope of the future for some people in a quite, personal way.
Recovery seems to be something that “occurs” rather than something that is “doable”.
and yes, a person does, and tries many many many things during recovery process..and than something “occurs”.
Someone used the analogy of a “switch” that went off with them.
I think it was SUZUKI that was asked:
“What is it like to be enlightened?”
and he replied;
“It is exactly the same as everyday life, except two inches off the ground.”
That may fit the sense of feeling of recovery.
A person may once again become extremely happy, sad, bored, depressed, ecstatic..experience the full spectrum of emotions again, without becoming derailed by feelings of wanting, or returning to the addictive way of life.
Again, this is not a pep talk per se, but it may be of help?
Hey Carlton
There’s another famous Buddhist axiom: “Before enlightenment, chop wood and carry water; after enlightenment, chop wood and carry water.” You can substitute “enlightenment” with “recovery” here too.
Recovery does “occur”; it has smushy boundaries until it gets stronger and better defined. It’s a process. But it doesn’t “occur” unless it is “doable.” I’m futzing with semantics here, but if I can’t see recovery(change) as a realistic, viable option, it ain’t gonna happen.
But I think all these things everyone is suggesting could work. It’s having all these options available so the addict can try them. When something sticks, that’s when it “occurs.” Recovery is also an experiment, but you wouldn’t think it, with the meager or “mono-dimensionality” of many treatment approaches.
For me, the “switch” was a different thing; that happened further into my recovery, and I think sometimes, for some people it never flips even though they quit using. But we know it when it does, and it feels like freedom.
Thanks, Carlton. Sorry for the rant. I’m not ranting at you, just ranting.
It’s true, people need to find out what works for them, and the more they intrinsically know themselves the better. In one of my SMART groups there’s a woman, who knows herself, and knows she can’t go cold turkey. It’d just be too much, and sabotage her ultimate goal of quitting altogether. So she’s got herself on a program where she doesn’t get drunk but has two glasses of wine max a night, if she wants them. She doesn’t really want to moderate, and she’s getting experience first hand about how hard it is to moderate for her, taking up almost as much mental energy as when she was drinking alcoholically. This is the experience she needs to have to understand herself, her motivation… to understand her own recovery…
One reply to that question, “what if it doesn’t feel like a choice?”, might be to stress what Marc calls self-programming. Point out that the freedom to choose diminishes as the addictive cycle progresses. The addict has the most freedom to choose when no using cues are present. Develop healthy habits of travel, association and self-care. Stay away from the old cues. CHOOSE the environment and daily habits to minimize exposure. However, when the first urge to use comes up (which it will, even with perfect self-programming), that’s when the addict must notice the shift, then CHOOSE to use the tools of recovery – distraction, substitution, connection – to get out of cycle. So, remind the addict that there is more choice early in the cycle. It might be helpful to deconstruct a real-life relapse story and find the early choice points that might have been easier to take advantage of. The relapse always starts before the relapse happens. That’s the approach I would take. It’s especially helpful in a group context – lots of stories to draw on.
All great strategies, Fred. I think he got more of this kind of support from his fellow detoxers (helping him see there’s a choice involved). I see all kinds of patterns of use, some where there doesn’t seem to be an option other than to get them out of the element. If the intention to abstain is not there, it’s pretty much impossible to stop. I think it’s important to get the user to recognize everyone has a distinctive use pattern, urge patterns and relapse and recovery patterns. And if they can start to recognize those patterns, and their emotional precursors on the horizon (like noticing and deconstructing their behavior chains). It’s important to look at what one is telling oneself, and recognize the emotions related to triggers, until they are more like objects separate from other emotions. Our emotional mind gets so tangled up in early recovery cuz we’ve been stuffing those feelings with substances. This is where mindfulness and meditation can be incredibly helpful
I agree very much. Mindfulness of one’s internal states is critical, as is willingness. Lacking either one predicts continuing problems.
Hi all;
Thanks for this Mark!!
I was just pondering this whole notion of addiction, addict, disease, disorder, dysfunction, denial, treatment vs voluntary remission or just giving the stuff up. I love this debate and its a real long time coming as you and many others allude to. I have not been blogging for a while now as I have been trying to work things out for myself as I had run, set up managed developed and designed treatment services for way over 2 decades now. I came to the scene via the scenic route institutions as a child, the streets, prison, gangs, DDU’s (the old drug dependency units) and semi concept houses, then full on concept houses then finally 12 step rehab in patient the old fashioned way.
I remember being told things like “my best thinking got me here” and whilst in my 12 step meetings that “my disease was out their in the car park doing press ups” and my personal favourite “if you use again you’ll die”.
So on reflection for me I had no one I was lonely, lost and very afraid so I was fertile fruit and I didn’t really have much of a mind of my own, never really learned back then that I could have wouldn’t know what it was, except I think part of the real me was my addiction a kind of “F The World and Everything in IT!!”. So I just supped it up and then went out into the world espousing the fuzzy logic I had learned (much in the same way me and my brain had learned to use as a way of not being able to face up to this big old scary world) I liked the get out clause of “the paradoxical nature of the 12 steps” which implied a cute reply to every question that was ever raised against it that didn’t make sense, example you keep what you have by giving it away? Really now lets look at that logically go give the next person every last penny you have in your wallet, walk away close it take it back out and look is it still there? well no! you gave it away!! Another great one was “minds are like parachutes they only work when their open” Perhaps you can answer that one Mark is there such a thing as a closed mind?
Anyway I have become detracted, what I wanted to talk about was the way I have changed the approach clinically to working alongside people as they attempt to work things out for themselves, which for me is phenomenological and experiential (or getting near to experience) it occurred to me in your latest book that you attempted to do just that and I really liked for the better part how well this was done. This in effect becomes part of the process of healing, or growing forward. The shared vulnerabilities of each story really highlighted the complexity of the human story uniquely different for each person and more importantly it managed this too for the story of addiction, or any other complex life experience. I am so glad you have begun to change the rhetoric but I am really keen to get in so I just wanted to share some of my own experience as well.
after 18 years of total abstinence I decided to go back to try drinking alcohol, I meant to see how it would feel to have this in my life, I have been fine for over 5 years now I am still here, not dead, not out kicking in doors or smashing out windows, or craving the insatiable and lustful desire for heroin, crack, speed or anything else remotely otherwise mood altering except I do suffer migraines and I will take opiate based painkillers on the odd occasion I get an attack (it works for me and that’s all that really matters). Instead and I must admit a few times I have gone overboard with alcohol, and suffered the next day uttering the words never again (thought I would never here that again). I am still a responsible member of society, a father, husband and I still help those in need offering what I can in their attempts to change. I have nothing and no special advice except to say we have a voice inside an inner voice it knows who we are and people have left us confused helping us to not listen to it and instead believing that we might be wrong, we are not! we always know best! our way wont make sense to everyone sometimes it wont even make sense to us until later (sometimes much later).
I guess I just wanted to add that I don’t think Addiction is a disease I have no evidence in my study, practice and in life that it is, sometimes it can look like it when a person is far from reach or the damage they have suffered is too great.
I think addiction a lot of the time is a really a quite normal response to our inner search for meaning and our disjointedness and disconnection with ourselves when things just don’t stack up, when things seem meaningless, or don’t make sense, when their is no apparent purpose and the absurdity of existence comes crashing home or our world feels like drabs and tatters around our very sense of self, or people hurt us and we cant make sense of it or we ask our-self whats the point but no answer comes back, then addiction makes good sense even when the histories we have offer no discernible or apparent hardship in our stories but inside we feel like our skin just doesn’t fit. Then addiction makes good sense and what is more it could happen to anyone, and probably to varying degrees it does in many ways. But addiction doesn’t have to be the only response… we do grow, change and make different paths.
I wonder how many people out there actually have a story of successfully recovering and their experiences become lost, because they don’t want to admit they have left this or that fellowship due to not wanting to be judged again?
I guess its time to stand up and be counted to let people know that you live life after addiction, childhood abuse, etc etc and not only live it but embrace it with all of it’s inherent uncertainties and lack of answers.
I wonder what a real experiential phenomenological treatment approach would like and would it be called treatment? I doubt it as that would only imply there was a pathology their in the first place.
Thanks Mark love your 2nd even more than the 1st!!!
And thanks to everyone else for their input.
Thanks for joining in. But you should know that shorter comments will be read by more people. It’s good to hear from somebody that going back to social drinking is available, possible, if not for everyone then at least for some. And it’s good to hear that, while it’s not a perfect ride, it can be pretty smooth overall. We see this in the statistics but it’s less common for people to talk about it personally.
I agree, as probably do many members of this community, that addiction is a normal response to people’s search for meaning. Of course it doesn’t help much, in the long run, except to shift the search to what’s inside rather than outside.
I’m really glad you liked the book, and especially the weave of the characters’ unique stories to get to the strange fusion between diversity and universality in addiction as a phenomenon.
CDL1, you wrote;
“I wonder what a real experiential phenomenological treatment approach would like and would it be called treatment? I doubt it as that would only imply there was a pathology their in the first place.”
Agreed, and to add to that, a very compelling and motivating element for recovery
can be witnessing recovery actually occurring.
When in the throes of an addiction, it is hard to believe a person could live without the
addiction, and unimaginable that the cravings and desire could ever change, but witnessing people recoving in there own way could help “crack the molds” of
mindsets, and lifestyles.
A recovery approach where there is an equal expectation of people both coming and going, due to having recovered, could help change the beliefs surrounding addiction, and throw new light on the understanding of Addiction and Recovery.
It is counterintuitive for an organization to see members leave, but knowing people come..and ALSO leave because they recovered, is a fundimental, and natural reason people would be attracted.
That “Source of Reference /Clearing House” idea that a few people posted about in the “Beginners mind” topic on this blog, could be the beginnings for that kind of recovery environment I think, and it wouldn’t be “treatment” as you say…
maybe call it an environment where “SIED’s” can possibly occur, or “Self-Inflicted Epiphanies and Discoveries” ?! 🙂
…to complete the thought, maybe call it a “Recovery Garden”, where
“Seid’s” of recovery can be planted to grow.
It may only need minimal amount of maintainance,..perhaps by ongoing individuals that experience the “flow” of people as they come and go.. this would reflect the nature of the environment itself, rather than become a “set in its ways” type thing?
Carlton, you say that, when in the throes of addiction, it’s hard to believe that it will ever rest, that the cravings will stop. I assume you mean hard to believe for both the addict and the social surround. I agree. In that sense, addiction really is a mind-set, a packed cluster of beliefs.
I like your description of the flow in an environment where people come in addicted and leave “in recovery”. That’s pretty much the description Johann Hari shares with us of the treatment programs in Portugal…very nonjudgmental, gradual, pressure free, essentially inviting change rather than demanding it.
A Hands-off approach that is based on individuals witnessing changes in beliefs, feelings, mindsets and lifestyles of fellow participants, could be the basis of an experiential phenomenological treatment approach.
Is that like the Portugal idea?
Another helpful element for recovery, would be a sense of life after addiction AND recovery.
Paradoxically, but yet naturally, when people recover, they rarely correspond to recovery sites and programs.
That may sound odd, but perhaps a definition of recovery is when you no longer have to do anything! 🙂
Here’s an interesting pilot study using TMS magnet tech on the brains of cocaine addicts …
http://www.alphagalileo.org/ViewItem.aspx?ItemId=158915&CultureCode=en
Looks promising.