
Two posts ago I promised to follow up on “what is addiction?” by supplying the missing piece. Anyone who has experienced addiction or studied it knows that compulsion is that piece — the elephant in the living room.
Here’s a quick review:
A key aspect of addiction, as we experience it, is the urge to complete the act, scratch the itch, etc. You’ve probably heard a dozen phrases that try to capture that feeling, that moment. We know we’re not going to feel any better, maybe worse, or if we are going to feel better it won’t last long. We’ve gone through all the arguments and  counterarguments as to why we should not, cannot, do it one last time. We have done all we can to steer a path home that avoids the liquor store, to wait until our dealer is out, to provide a context that makes it unattractive or even impossible, like going to a meeting even. And then we lunge for it. The behavioural switch has been switched on — so it seems. And the alternatives and obstacles fade into the background. Just do it. Get it over with. There’s still 15 minutes before the liquor store closes. We can still find our dealer if we try.
counterarguments as to why we should not, cannot, do it one last time. We have done all we can to steer a path home that avoids the liquor store, to wait until our dealer is out, to provide a context that makes it unattractive or even impossible, like going to a meeting even. And then we lunge for it. The behavioural switch has been switched on — so it seems. And the alternatives and obstacles fade into the background. Just do it. Get it over with. There’s still 15 minutes before the liquor store closes. We can still find our dealer if we try.
This compulsive aspect of addiction arises over time. It’s not there for the first few weeks, or months, or maybe even years. And then it’s the main act. It’s the Achilles’ heal that resists every effort at mindful self-control. So it seems. And resisting the urge just wears us down — as per my descriptions of ego fatigue, in my book and other writings. The anxiety that mushrooms as we continue to resist becomes agonizing.
We can trace this psychological and behavioural sequence in ourselves or others. Both at the minute-by-minute scale — the way it builds over the course of an afternoon — and the month-by-month scale, the way it gets stronger the longer we continue using. But what’s going on with the brain in parallel?
The launching of an action (toward a goal) is governed by the striatum (or basal ganglia), a large structure with connections both “downward” to the amygdala and other parts important for emotion and “upward” to the prefrontal cortex, where expectations, plans and choices are activated. The striatum has a ventral (“southern”) terminal, which we often refer to as the nucleus accumbens. That’s considered the hot  spot for addictive cravings. But it’s also got a dorsal (“northern”) region. While the ventral striatum evokes anticipation, longing, and zeroing in on potential rewards (e.g., drugs, booze, porn), the dorsal striatum seems to be involved in automatic behaviours — what psychologists call Pavlovian conditioning, or stimulus-response (S-R) events.
spot for addictive cravings. But it’s also got a dorsal (“northern”) region. While the ventral striatum evokes anticipation, longing, and zeroing in on potential rewards (e.g., drugs, booze, porn), the dorsal striatum seems to be involved in automatic behaviours — what psychologists call Pavlovian conditioning, or stimulus-response (S-R) events.
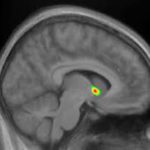 I’ve written about all this stuff previously, so I won’t get into more detail here. The main point is that only the ventral striatum (southern region: nucleus accumbens) becomes activated (bright yellow spots on the MRI) in early addiction — e.g., the first few months. But in later-stage addiction, activation increases in the dorsal striatum. For a while addiction neuroscientists thought that the addictive trigger got passed along, so to speak, from the ventral to the dorsal striatum. That could explain how addiction seems to evolve from being an active desire, motivated by an expected good feeling, to a habit, beyond conscious control and motivated by nothing at all — purely automatic. In fact, the disease model of addiction — the idea that drugs hijack the brain and destroy the will — got a lot of traction from this kind of neural model. See, folks, addiction means no more choice — it’s simply a compulsive act that can’t be stopped.
I’ve written about all this stuff previously, so I won’t get into more detail here. The main point is that only the ventral striatum (southern region: nucleus accumbens) becomes activated (bright yellow spots on the MRI) in early addiction — e.g., the first few months. But in later-stage addiction, activation increases in the dorsal striatum. For a while addiction neuroscientists thought that the addictive trigger got passed along, so to speak, from the ventral to the dorsal striatum. That could explain how addiction seems to evolve from being an active desire, motivated by an expected good feeling, to a habit, beyond conscious control and motivated by nothing at all — purely automatic. In fact, the disease model of addiction — the idea that drugs hijack the brain and destroy the will — got a lot of traction from this kind of neural model. See, folks, addiction means no more choice — it’s simply a compulsive act that can’t be stopped.
 That turns out to be inaccurate. Recent studies, both with addicts and with those suffering from OCD (which has lots in common with addiction), show that the ventral hot spot, the nucleus accumbens, remains part of the flow of activity that moves us from a stimulus (a rumbling in the gut, a vodka ad, a
That turns out to be inaccurate. Recent studies, both with addicts and with those suffering from OCD (which has lots in common with addiction), show that the ventral hot spot, the nucleus accumbens, remains part of the flow of activity that moves us from a stimulus (a rumbling in the gut, a vodka ad, a  phone call from a buddy) to a response. The response. The data suggest that the ventral and dorsal striatum both get involved in the kind of compulsive actions that characterize addiction. But they seem to take up different phases of the moment-to-moment sequence, with the dorsal striatum staying active longer, holding the action “at ready” until it’s executed, and the ventral striatum contributing to the earlier phase, the blush of wanting and seeking.
phone call from a buddy) to a response. The response. The data suggest that the ventral and dorsal striatum both get involved in the kind of compulsive actions that characterize addiction. But they seem to take up different phases of the moment-to-moment sequence, with the dorsal striatum staying active longer, holding the action “at ready” until it’s executed, and the ventral striatum contributing to the earlier phase, the blush of wanting and seeking.
So the habitual nature of addiction is nothing like the habit of wiping your hands on a napkin or brushing your teeth. It’s not automatic in the same way. Addictive urges are far more complex. Even after years of addiction, those compulsive moments are packaged together with an emotional surge, a bouquet of emotions that are probably both positive and negative, a conscious sense of moving toward an expected reward, AND, finally, a more automatic sense of “must.”
What’s the point?
If the compulsive aspect of addiction remains part of a conscious stream of anticipation and preparation, then we have far more choice than we might have thought. Choice and will don’t just disappear with years of use.
Certainly the compulsive “just do it” urge increases over time, both over months and years and over minutes and hours. But the compulsion never replaces the impulse, the wish, the want, the conscious anticipation that we associate with the nucleus accumbens. Rather, the compulsion might be the final springboard to action, coming at the tail end of a series of thoughts and feelings that are conscious — and therefore controllable.
Comments
34 responses to “Okay, what about compulsion?”
I guess you nailed the complexity of it here the reason why it will never be anything other than complex, individual and unique in its experienced and existence bound sense. It is also clear through this lease why this knowledge is set to drive up confusion and discomfort when placed in a context that is medically bound to look at symptom and cure.
The conundrum here is there’s no cure to being human, in the final analysis there is no them and us, addict or non addict, disease or non diseased! there is only the complex and universally mystery of lived experience through the vacuum of context which is ultimately as unique as each fingerprint.
So the good news is there’s nothing abnormal about addiction per say (not the same as harmful here pointed out for those who think I am undermining its devastatingly destructive potential!). There is only an emerging curiosity and spontaneity as to its utter normalcy.
Love your work Marc a breath of fresh air thank CM
Thanks, CM. Indeed there is nothing really abnormal about addiction. But I think it appears close to the nasty end of the scale when it comes to human suffering, mainly because of the conflicts it induces when we try to choose between compelling alternatives.
CM, Marc, to newcomers, realizing that addiction is not abnormal could be of great help and valuable to realize.
I would venture to also say that “compulsion is compulsion”.
For instance:
The compulsion that drives a person to go against all common sense and brave bullets to raise a fallen flag in battle, is same compulsion that drives a person to plot, plan, and maintain an addiction.
“This must be done at all costs”, as it were.
Put this way, the shame and guilt many newcomers feel could be alleviated. and they could get a helpful and valuable “leg up” in their individual recovery process.
Excellent! Thanks you!
Marc, Personally, I found the feelings of compulsion and desire for an addiction can, and do, change, and controlling them is NOT the issue for keeping the addiction at bay.
For instance,
A it is a given that a person’s deep and life-changing feelings rarely change for certain things, such as a favorite family member, certain writers, film directors, composers, sports teams, etc.
But it is also true that sometimes these long-time and deep-seated feelings can change.
Most people can relate to realizing that at some time they no longer sought out new publications of a favorite writer, stopped checking concert tour dates, movie schedules, stadium games,
Being in NYC, I asked a SMART group if anyone could imagine if their feelings for the Yankees or the Mets would ever “Change”.
The knee-jerk reaction was shock, but it made the point that feelings that seem permanent and unimaginable can and do change.
Correction!
The first sentence should read:
Marc, Personally, I found the feelings of compulsion and desire for an addiction can, and do change, and controlling them is NOT the issue for keeping the addiction at bay.
Two comments, Marc. First, I sometimes asked patients to imagine they were walking down a street, desperate for a drink and suddenly saw the only bottle-shop in town on the other side. Would they still cross the road if a machine-gun were permanently firing down the middle of the street? Of course not, they replied, except for a few jokers who said it would be a good way to end it all. Disulfiram, I would then suggest, works in a similar way.
A recent New Zealand study noted that disulfiram effectively removes one of the most annoying features of being an alcoholic – the endless internal arguments and conversations that patients have with themselves almost every minute of the day about whether they should or shouldn’t drink. Some patients described it “in terms of an incessant internal homunculus that demanded alcohol”. Disulfiram replaced those endless ruminations and temptations with “a life-world where alcohol is simply no longer an option”. One patient described how, when he wasn’t taking disulfiram, he was “always tossing up whether I should drink or not. And I list all the pros, all the cons, but at the end of it, I just go ‘fuck it, fuck it’… When I’m on Antabuse, it’s just like. Well, I can’t”. Naltrexone – especially depot naltrexone – works the same way for opiates.
Similarly, most of the recurrent alcohol-related offenders in Instant Justice programmes – who include many people who are undoubtedly alcoholic – don’t seem to find it difficult to give consistently negative breathalyser tests if the penalty for a positive one is instant imprisonment for just one night, so that they can still stay in work.
All this indicates more self-control than your piece suggests and once people get used to walking past dealers, pubs and bottle-shops for a few weeks, it become progressively easier to do so without medication eventually The German OLITA study showed that that ‘eventually’ sometimes meant 18 months of continuous medication to achieve their remarkable 50%+ abstinence rate 9 years later in a group of very chronic treatment-resistant alcoholics.
Hi Colin. That’s a very useful perspective, and certainly disulfiram and naltrexone help people by cutting through the internal dialogue…because it’s no longer viable. But I don’t think my piece points to a lack of self-control. In fact, the opposite. I was thinking that my analysis suggests greater self-control is possible, even when people might feel that their behaviour is automatic. In other words, the implication of the neural research might be that the old view of addiction as pure compulsion is way too narrow.
That’s the big leap though to a paradigm embracing that there actually is a choice despite feeling, believing, experiencing that there is not something that the disease, (automaticity, implicit identity) models positions actually reinforce.
I agree with the choice theory but from the internal lense of those in the grips of a crippling and destructive compulsively obsessed driven addiction it’s unlikely to feel like that? I guess for me it’s the chasm that sometimes feels unbridgeable and frustratingly and ironically only understood and accepted from the other side of the experience.
To clarify it’s more easy for me to buy it after being outside of my addictions for 26 years but I would never have agreed with it when I was in the grips, that would have felt too scary! to actualy think and know and believe I had a choice, a hand in the misery I caused myself and those around me.
That’s where the disease model worked for me until eventually and thankfully I grew up (existentially) and could look myself square in the eyes and let the dice fall where they would without need for shame, blame or lack of personal responsibility.
Nothing to be ashamed of just grateful to be free and to see the experiences for what they where and not a moral failing or a perfunctory absence of wanting a better way to live but not knowing ho? Addiction is not a blot on my personhood and the only certainty there is, is change itself. CM
Hi CM. You said a lot here. It’s true that when we are in the thick of it, it feels that there is no option. That is, it feels like what they call a singularity. But it can be dissected and opened up. As you say, one way to do that is to grow up and look back. Another way might be to enlarge the range of choices available at that moment. I remember the feeling well: there were no other choices. That’s the singularity that needs to be exploded, understood, reflected on. It is certainly possible. So many of us have done it.
Absolutely in every sense a widening of belief that all those self defeating addiction reinforcing narratives loosened with a true knowledge that we can overcome. Sadly I guess too many believe the singularity and crawl back inside the addiction. It’s frustrating if only we could get through help them believe then maybe so many need not die. Really sad but paradoxically really positive. Keep fighting the good fight my friend✌️
“Well it seemed like a good idea at the time”
I agree that there is always a choice but it seemed in retrospect that all the good ones were hidden from my immediate view or that at the time all the irrational ones were more easily rationalized as well as the inverse.
Exactly! See above.
This i excellent Marc as usual and really clarifies it . But also leaves me hungry for a practical solution
As I see it many come for help feeling they no longer have a choice but what you and others have mentioned, an early step is to help the person see that they actually do — not easy mind you but doable.. And if they can make one simple ones they gradually see that it actually can be done
The disease model really precludes this sort of approach .. it would be the only disease I know of which you choose to have and then find that you can choose not to have it anymore .
Hi Bill. This seems to be the theme of the comments so far. Yes it’s supremely hard to open up that moment and convey the reality of choice. One thing I have tried to do with clients in therapy is to go easy about cutting down, controlled use, etc. That way They are not choosing between the devil and the deep blue sea. And then, as you say, once one choice is made, the next step doesn’t seem so impossible.
Marc,
Years ago, a fellow SMART Facilitator described this following “mirror” technique for opening up that moment to convey the reality of choice;
Before he would go to the liqueur store, (or dealer, website, etc), he would go into the bathroom… look in a mirror at himself and say:
“Ok… I am now going to go out of the door and get_____.”
It can create a buzz of fun at a recovery meeting, but this simple, instant and graphic technique is quite compelling.. and self-applied too.
Note:
This was before cell-phones had cameras, so possibly a person’s own
cell phone camera could serve the same purpose?
Marc, Interestingly, most meeting attendees later reported that just recalling the IDEA of this mirror technique opened up that moment to convey the reality of choice.
I work with teens a bit at a recovery high school. One exercise that engages them is to deconstruct their usage (because neither I nor they believe they are addicted yet. More like “habituates” than addicts”). We go around the room and everyone states their drug of choice, what it does for them, when do they want to do it and why, and what happens.
Even at the very beginning kids, who are trying to establish their social identities, can realize that when “it seems a good idea at the time,” and have a little epiphany about themselves. In other words, even teens can think it through if they can slow themselves down enough to check their motivation with potential and evidential outcomes. It takes practice to see it coming in the moment…
Same for adults. People come to understand what’s driving their compulsion in their own time, when they’re ready. But it’s important to notice whether you’re ready or not.
Matt, thanks for translating my rather abstract thesis into pragmatic steps. Yes, slowing one self down is critical. Yes seeing the moment coming before it arrives is also critical. Great advice.
That’s one reason why mindfulness practices can be so helpful in recovery. When one is paying attention to the activity of their own mind, they can begin to recognize the space between thoughts and other automatic mental activity, and in that distance have the opportunity to make a different decision.
Matt,
Yes, paying attention to the activity of ones own mind can help “crack the mold” that you are a helpless, hopeless addict.
One early realization can be that “slips” and relapses are NOT accidents.
for instance:
“Oops, I slipped and don’t know what happened”, can eventually become something like:
” There was a powerful compulsion to re-depend on the addiction, so I made a decision… and chose to seek, obtain, and actively re-engage with the addiction.”
It is a mouthful, but in short, the reality went from;
“I don’t know what happened”
to;
“I know what happened”.
It can be an early and valuable realization.
https://www.orangeville.com/news-story/7334183-an-orangeville-mother-hopes-her-son-s-fentanyl-overdose-death-will-help-other-parents/
Types of Facilities
Compulsion becomes similar to the schizophrenic dissociation (I did it because I heard voices, but it was not me). I think addiction changes the brain for good, making it more difficult to recover. The once addicted can become free from addiction, but would have a lower trigger threshold than prior to addiction.
In some cases chemical and food sensitivities make the person inclined to addiction. They cause pain and the person tries to calm the pain with whatever is calming (alcohol, drugs, sport, religion etc.). He/she than becomes addicted to the calming tool of choice. In such a case, one would have to resolve the environmental and food sensitivities first: elimination and rotation diet; clean environment. If the offending stimulus can not be avoided, nutrients can help.
Another situation that is contributing to addiction to drugs is the high sugar diet. Dr. Nicole Avena has done a lot of research in this area.
Just wondering whether or not you have actually experienced addiction first hand or is all of your knowledge from books and other people’s experiences? To me (someone in recovery), the most powerful knowledge bases for input on addiction are a) those who have been there themselves. They seem to be very empathetic b) individuals who have research this disease and c) those who have listened to the experience of others. There are too many “experts” on addiction who have absolutely no idea what addicts go through during addiction and on their road of recovery. You seem to have a lot of knowledge about addiction. It is evident in your posts. That is great. I just have a hard time with someone telling me all about addiction when they have not experienced it themselves.
Seriously? Do a bit of homework….
Marc, I owe you an apology. I had not read your bio before my last comment. Please forgive me. We all need to come together to supply an accurate message about addicton and recovery to those who still suffer and those who care about the suffering.
No problem, Michael. It’s a bit narcissistic of me to think that everyone commenting on this blog knows my history. Sorry for my snappy response.
Yes, this blog represents converging perspectives, opinions, and understanding. Welcome aboard!
Mike, I would never speak for him, but suffice to say that Marc thoroughly satisfies all a, b, and c of your criteria for having the right to comment on addiction. And while I agree that it is often difficult for those who have absolutely no experience with the power of compulsion that accompanies addiction and physiological dependence (especially those narcotics and alcohol) to relate to the experience of those of us who have, don’t let that invalidate their input. This is especially true of scientific research into the physiological and neurological aspects of the phenomenon. The addiction industry is fraught with close-mindedness and rigidity when it comes to new insights and paradigms. I did find that a little rigidity did help me in the beginning of my healing from my own addiction, as I was battling some unbelievably strong internal forces (which I assume you can relate to), but as I became more comfortable with abstinence, I realized that there is a lot more to the story. I am so glad that Marc (and a handful of others–not all of whom have experienced traditional addiction) are having these conversations, even if they sometimes run into conflict with certain commonly accepted “truths” that have been in practice for too long in the field.
Thanks, Eric. What you said about not invalidating contributions from different sources is really important. I know a guy who’s never been addicted to anything, as far as I know, whose only contact with addicts is with small furry ones who live in cages, who spends his days looking at numbers rather than sharing anecdotes, and yet who knows more about addiction than almost anyone else I know. His name is Kent Berridge.
Made me look up Kent Berridge. incentive salience…..cool stuff
Very!
Marc, your words “lunge” and “must” stand out. “Must lunge!” “Where / when / how / what / who is my next fix?” Compulsion is a terrible thing. The feeling: being driven from deep within by a maniac driver in a vehicle with no brake. Even when the substance/process offers temporary relief from the frenzy, the underlying mechanism is still roaring and rumbling, like a rocket still tethered to the launch pad during those pivotal ten seconds before it’s released. Full throttle and full stop at the same time. Quietude, neural serenity, even an iota of calm — impossible. The drivenness is agony, and until there is some sense of relative safety and a small modicum of internal regulation/self-soothing inside the person, and some small sense of being bonded with something/someone other than what is deranging us, the engine will continue to roar until it blows. Half of my original family were addicts — all dead, all driven to their deaths by that horrific compulsion.
I keep thinking of pages 294-295 in your memoir — that “wisp of self-love” you felt, and the voice within you that suggested the possibility of saying no. A shocking, alien tinge of mercy and spaciousness — breathing space.
I often play with the AA mantra, “One step at a time.” Often, it’s one breath at a time. One thought at a time.
Gandhi, too: He said, “Be the change you wish to see in the world.” I say, sometimes with every ordinary action, “Be the change … Be the change … Be the change …”
It’s somehow about softening, taming, gentling the compulsion. Somehow slowing the monstrous engine before it blows up. Somehow, taking one breath at a time.
Somehow, a wisp of self-love.
Hey Marc,
Read both of your books while in rehab (separate times), last being time number seven I think? It’s funny I stumbled across this post because it is exactly what I am going through and usually my downfall after being sober for a while. Drank the day before being clean for a year and was stuck in the muck for about two and a half months afterwards. Now, after a less than great relapse my thinking has returned to much of the same; I have made sure to have zero accountability with anyone and that my choices in life are respected. Essentially, I have unlocked the gate and am free to choose how I view myself, others and the world – and I want to drink. Not because I am upset with myself or anyone else, but because I can. I want to view myself as normal, being able to fit into patriarchal society and be apart of the status quo. Perhaps that is large part of it? People who just don’t seem to fit in because they are different, and generally like to play by their own rules or rules that they agree with. I have talked to A LOT of addicts and a common thread amongst them seems to be crime and the maintaining of an image presented to us through media outlets, it’s sad. People have to deny themselves who they are and what they want to be/do because:
1) It’s expensive and exclusive
2) We are scared and lack proper motivation
3) It challenges the rigidity of established structures be it “recovery” or not
I personally want life a completely different way than what I am presented and the feeling of being deflated when it comes to changing course is really tough to deal with, as most of us know – the resources are just not there.
I could go on and on, I’m done for now – lol /end rant
I hope at least some of that made sense,
keep up the good work Marc, thanks!