Response to the heroin epidemic: 1. Methadone and harm reduction
The heroin “epidemic” is a major concern all over the world right now. What are the various philosophies for dealing with it? In today’s post I’ll share some impressions from my recent visit to a harm reduction/methadone clinic in Belgium. Then I’ll post a piece by Percy Menzes who is dedicated to the use of naltrexone and policies that minimize access. Then we’ll see what Sally Satel has to say about programs that use punishments and rewards to get people to quit — so called incentives. That should keep us busy.
Last Thursday I took a train to a town in Belgium called Diest. It was two or three days after the attack on Brussels…so there were quite a few military guys standing around in the train stations with machine guns in their hands, ready for action. Not exactly reassuring.
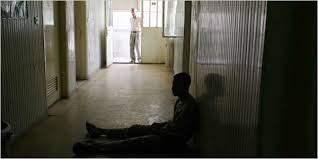
But with all the chaos and pain that seem to infest the world right now, I felt a warm, cocoon-like embrace when I entered the Wit Huis (The White House), a harm reduction clinic that provides  prescriptions for methadone, counselling, and a place to hang out for a little while.
prescriptions for methadone, counselling, and a place to hang out for a little while.
The waiting room was a pleasant lounge where people (mostly addicts) could relax with tea and cookies (and baked goods such as Easter cakes) and chat with their fellow travellers. It was clean, bright, and there was an air of positive energy: care, concern, and understanding. There were leaflets everywhere, outlining the dangers associated with different drugs. And there was always  a staff person present, just being friendly, chatting, offering snacks. The staff consists of two social workers, two MA level psychologists, a criminologist (to help with charges, probation, as so forth), and the doctor, Carl, who wrote the methadone prescriptions. Carl was my host.
a staff person present, just being friendly, chatting, offering snacks. The staff consists of two social workers, two MA level psychologists, a criminologist (to help with charges, probation, as so forth), and the doctor, Carl, who wrote the methadone prescriptions. Carl was my host.
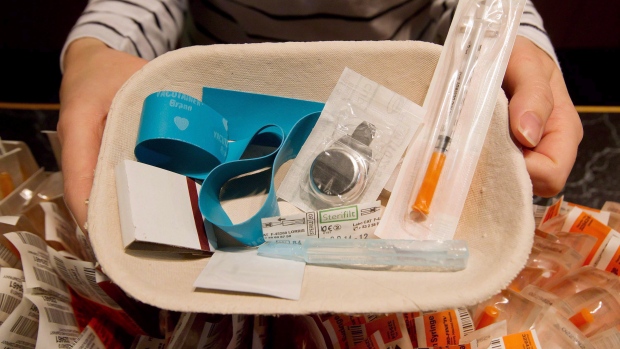
After being shown around — rooms for counselling, a play area for people with kids, a laundry room, showers, a medical area where wounds and infections were treated and clean needles and accessories were handed out  (in exchange for used needles) — I mostly sat in a chair next to Carl in an office/interview room, while one client after another came for their methadone script. It was sort of fascinating.
(in exchange for used needles) — I mostly sat in a chair next to Carl in an office/interview room, while one client after another came for their methadone script. It was sort of fascinating.
Most were heroin addicts of course, but many also used meth and/or coke. Many of the heroin users balanced their methadone dose with heroin obtained on the street. And this was no secret. There wasn’t much lying or sneaking going on, according to Carl and the others. It was a tacit assumption that opioid addicts would fluctuate in when, whether, and how much heroin they used to spice up their diet. And there was no confrontation. There was no scolding, no pep talks, no condescension, no sense of a parent figure keeping tabs on the naughty children. Yet Carl was careful to balance the dosage of methadone against simultaneous heroin use: less methadone with more heroin, naturally, to minimize the odds of overdose. And overdose was rare with this population. So how did they manage that?
The clients seemed content to report honestly on what drugs they were taking, mostly because there was no censure or disapproval, either explicit or implicit, in the attitudes and behaviour of the staff — including Carl. But just to make sure, unanticipated urine tests were requested when people said they’d stopped using heroin and wanted to increase their dose of methadone to compensate. Again, it was the warmth and camaraderie that flowed between staff and clients that neutralized the temptation to lie. The smiles and hand-shakes, the invitations to chat about how things were going, the absence of demands. These people were leading lives that to some extent they were choosing and to some extent they were stuck in…and nobody was judging them. The purpose of the clinic was to keep users safe, healthy, and out of jail.
Nevertheless, despite all this sweetness and light, these folks were seriously addicted, both physically and psychologically, to a very powerful drug. They weren’t anywhere close to safe and stable in the big picture. About half were homeless, which generally meant they slept in different homes night by night, or in abandoned houses, or with relatives. They were not the happiest of campers.
And where I saw this most clearly wasn’t in the statistics — re homelessness, unemployment, co-occurring psychiatric disorders — but in the posture and facial expressions of the people sitting  in the chair across from the doc. They often looked defeated and helpless. While some expressed enthusiasm, plans for the future, many looked dreamy or blank. Quite a few had the hunched over posture that expresses shame or remorse. Their eye contact might be sparse and fleeting, looking down a lot — the gaze pattern of people who live with a chronic level of shame or sense of inferiority. A sense of personal failure they’ve grown deeply accustomed to.
in the chair across from the doc. They often looked defeated and helpless. While some expressed enthusiasm, plans for the future, many looked dreamy or blank. Quite a few had the hunched over posture that expresses shame or remorse. Their eye contact might be sparse and fleeting, looking down a lot — the gaze pattern of people who live with a chronic level of shame or sense of inferiority. A sense of personal failure they’ve grown deeply accustomed to.
That part was sad. That aspect made me think that harm reduction and methadone provide a solution to the heroin epidemic, but it’s not a great solution. Something is still seriously wrong here, and this form of treatment, connection, and care can make it livable. But only just.
Clinics of this sort have sprung up in towns and cities throughout Belgium and other European countries. As always, I’d love to hear your opinions.



 xclusion from evaluations of how they’re doing, what they’re doing, and when they’ve had enough. At the outset they are told, “We’ll have to break you down so we can build you back up again”—a phrase commonly heard in institutional settings, according to Matt Robert, a friend, former addict, and group facilitator in both institutional and community-based programs. It’s not that such policies are borne of ill intent. It’s just that they’re wrong-headed. Disease model advocates like
xclusion from evaluations of how they’re doing, what they’re doing, and when they’ve had enough. At the outset they are told, “We’ll have to break you down so we can build you back up again”—a phrase commonly heard in institutional settings, according to Matt Robert, a friend, former addict, and group facilitator in both institutional and community-based programs. It’s not that such policies are borne of ill intent. It’s just that they’re wrong-headed. Disease model advocates like 



 Informed by unparalleled neuroscientific insight and written with his usual flare, Marc Lewis’s The Biology of Desire effectively refutes the medical view of addiction as a brain disease. A bracing and informative corrective to the muddle that now characterizes public and professional discourse on this topic.” —Gabor Maté, M.D., author of In The Realm of Hungry Ghosts: Close Encounters With Addiction
Informed by unparalleled neuroscientific insight and written with his usual flare, Marc Lewis’s The Biology of Desire effectively refutes the medical view of addiction as a brain disease. A bracing and informative corrective to the muddle that now characterizes public and professional discourse on this topic.” —Gabor Maté, M.D., author of In The Realm of Hungry Ghosts: Close Encounters With Addiction
Recent Comments